$500.00
We have taken video from the live 15-hour lecture and lab course including Power Point slides, demonstration, lab, and audience question and answer sessions. This home study course is available online/digital which allows for viewing in the comfort of your home or office. You will have 21 days to complete the home study from the time you receive online access.
This advanced lecture and lab course explores the biomechanics of contralateral and ipsilateral myokinematic lumbo-pelvic-femoral dysfunction. Treatment emphasizes the restoration of pelvic-femoral alignment and recruitment of specific rotational muscles to reduce synergistic predictable patterns of pathomechanic asymmetry. Emphasis will be placed on restoration, recruitment, and retraining activities using internal and external rotators of the femur, pelvis, and lower trunk. Guidance will be provided on how to inhibit overactive musculature. This will enable the course participant to restore normal resting muscle position. Participants will be able to immediately apply PRI clinical assessment and management skills when treating diagnoses such as piriformis syndrome, ilio-sacral joint dysfunction, and low back strain.
Education Level: Advanced

Session 1: Introduction, Left AIC Pattern, Pattern vs. Position, Biomechanical Influences of the Femoral-Acetabular Joint, Lumbo-Pelvic Joint Dynamics, Femoral-Acetabular Joint Dynamics, Ligamentous Muscle
(134 minutes)
Session 2: Femoral Internal and External Rotators, Positional and Compensatory Influences of the Left AIC Pattern on Muscle of the Lumbo-Pelvic Femoral Region, Myokinematic Coloring Section
(85 minutes)
Session 3: Desirable “Real Estate” for Repositioning, Hole Control, Myokinematic Influences on the Pelvis & Femur, Myokinematic Restoration Examination Tests and Assessment
(123 minutes)
Session 4: Myokinematic Restoration Examination Tests and Assessment (Lab), Myokinematic Restoration Repositioning, Soft Tissue Pathology and FA ROM Treatment Rationale
(138 minutes)
Session 5: Myokinematic Functional Relationships, Hruska Adduction Lift Test
(120 minutes)
Session 6: Hruska Adduction Lift Test (Lab), Treatment Considerations and Myokinematic Hierarchy for the Non-Pathologic Left AIC Patterned Patient
(99 minutes)
Session 7: Treatment Considerations Using the Hruska Adduction Lift Test (including lab)
(162 minutes)
Session 8: Case Studies, Myokinematic Restoration Inhibition Programs, Left AIC Related Pathomechanics
(102 minutes)
Muscular Structures of the Pelvis
IC Adductor (Ischiocondylar portion of the adductor magnus)
Internal and External Femoral Rotators
Lower Half Pelvic Musculature (Gluteus Maximus, Levator Ani, Coccygeus, Pubococcygeus, Adductors, Obturators)
Upper Half Pelvic Musculature (Piriformis, Gluteus Maximus, TFL, Psoas)
Ligaments
Sacroiliac Ligaments (anterior/posterior) Anterior Ligaments: Iliolumbar, Sacrospinous Posterior Ligaments: Interosseous, Long Dorsal, Sacrotuberous
Femoral Acetabular Ligaments: Iliofemoral, Pubofemoral, Ischiofemoral
 Anterior Interior Chain (AIC)
Anterior Interior Chain (AIC)
Muscles: Diaphragm, Psoas, Iliacus, TFL, Vastus Lateralis, Biceps Femoris
Opposition Muscles: Hamstrings, Gluteals, Internal Obliques
There are two anterior interior polyarticular muscular chains in the body that have a significant influence on respiration, rotation of the trunk, ribcage, spine and lower extremities. They are composed of muscles that attach to the costal cartilage and bone of rib seven through 12 to the lateral patella, head of the fibula and lateral condyle of the tibia. These two tracts of muscles, one on the left side of the interior thoraco-abdominal-pelvic cavity and one on the right, are composed of the diaphragm and the psoas muscle. With the iliacus, tensor fasciae latae, biceps femoris and vastus lateralis muscles this chain provides the support and anchor for abdominal counter force, trunk rotation and flexion movement.
FA = Femoral Acetabular (femur moving on the acetabulum)
AF = Acetabular Femoral (acetabulum moving on the femur)
Left AIC = Left Anterior Interior Chain
FA IR = Femoral Acetabular Internal Rotation
AF IR = Acetabular Femoral Internal Rotation
The patient lies on his or her side with the lower leg and hip flexed (90 degrees). Stand behind the patient and passively flex, abduct and extend the hip to neutral while maintaining 90 degrees of knee flexion. Passively stabilize the pelvis from falling backward and allowing femoral internal rotation to occur. Make sure the top innominate is positioned directly over the bottom innominate so the frontal plane starting position does not give any false positives (top innominate too cephaled) or false negatives (top innominate too caudal).
A positive test is indicated by a restriction from the anterior-inferior acetabular labral rim, transverse ligament, and piriformis muscle or impact of the posterior inferior femoral neck on posterior inferior rim of acetabulum that does not allow the femur to adduct; possibly secondary to an anteriorly rotated, forward hemipelvis. Usually seen on the left especially if left Extension Drop Test is positive in a Left AIC oriented patient.

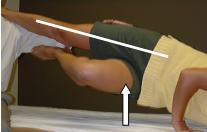
The patient is positioned in supine with both thighs on the table. Both hips and knees are flexed to the chest. Passively lower one leg over the edge of the table while helping the patient hold the untested knee close enough to the chest to maintain the low back against the table. Do not allow hip abduction to occur past zero degrees on the tested extremity while passively dropping the FA joint into extension.
A positive test is indicated when the tested lower extremity (usually the left) is restricted in hip extension because of the forward orientation of the tested side compared to the other. If both femurs do not approach the edge of the mat or table the patient is tested on, the innominates are rotated forward bilaterally and the psoas muscles are on slack. Placing the femur in “neutral” is actually placing the patient’s femur in external rotation. This tightens the TFL and VL and restricts hip extension.
There is also a rotary component to this issue, especially seen with limitation in hip extension on one side. Since the forward, anteriorly rotated pelvis accompanies sacral rotation to the contralateral side (right rotation on a right oblique axis or left rotation on a left oblique axis) the iliofemoral ligament will also limit extension when the femur is externally rotated by the therapist, through testing with the femur in a “neutral” position.
The femur in this case will not approach the patient support surface without femoral internal rotation and or through luxation (i.e., “click”) of anterior superior femoral head moving forward under the superior anterior condyloid labral rim of acetabulum.

The patient is positioned supine with knees maximally flexed and together, and feet flat on the table. Passively rotate the legs to the trunk’s resting state with one hand, while stabilizing the trunk with the other hand (placing it on the anterior lower ribs and sternum). A yardstick may be used to measure the distance from the mat to the upper-most point of the superior knee, while maintaining the opposite posterior thorax contact with the mat. Repeat the test in the other direction.
A positive test is indicated when the legs do not rotate in one direction as compared to the other. For example, the legs are restricted in rotation to the left (i.e., the legs do not rotate to the left as they do to the right as measured through the use of an upright ruler). This means that trunk rotation is limited more to the right secondary to probable left hip anterior rotation and sacral-lumbar orientation of the spine to the right. Therefore, postural restoration should be initiated at the left lower extremity to address left mechanical instability and maintain proper restored pelvi-femoral neuromechanics.

This test is used as a Myokinematic measurement with each grade reflecting muscle position, strength, and neuromuscular ability. The test is named for the leg, which is placed on the examiner’s shoulder. (Patient is lying on their right side with left ankle placed on examiner’s shoulder – “Left” Hruska Adduction Lift Test.)
Position
Patient sidelying – back rounded
Uppermost lower extremity resting on therapists shoulder (neutral hip, extended knee)
Lower leg in flexed position
Maintain pelvis in a neutral position (do not allow upper pelvis to rotate forward or backward)
Mechanics
Step 1: ask patient to raise ankle of flexed lower leg to upper knee
Step 2: have patient raise flexed lower knee while keeping ankle to the knee
Step 3: patient will then raise lower hip while maintaining the above positions
Discontinue test at the step patient is unable to perform
Grading Criteria
LEVEL 0
Inability to raise lower ankle off mat or table.
Obturator weakness of flexed extremity.

LEVEL 1
Ability to raise lower ankle to upper knee.
Inability reflects either weakness of FA external rotators or AF stability of active extremity.

LEVEL 2
Ability to raise lower knee and ankle.
Inability reflects instability of AF and weakness of adductor magnus and obturators or an anterior tilted and forwardly rotated pelvis with accompanying FA IR weakness secondary to long position of ischiochondylar adductor and short position of gluteus minimus, medius and TFL.

LEVEL 3
Ability to maintain above position while lifting lower hip off table slightly.
Inability reflects weakness of FA stabilizers on extended extremity including the short head of the biceps femoris and adductor magnus and possibly bilateral AF stabilizers including muscles of the pelvic diaphragm and lower gluteus maximus.

LEVEL 4
Ability to raise hip completely off mat or table to level of patients shoulder and examiner’s shoulder.
Inability reflects lack of core lumbopelvic femoral strength and more than likely the internal obliques on side of extended leg and external obliques on side of flexed leg.

LEVEL 5
Ability to raise hip above level of the patients shoulder and equal to examiners shoulder.
Inability reflects patient’s strength and neuromotor proprioceptive skills to shift hips.
This test is used as a Myokinematic measurement with each grade reflecting muscle position, strength, kinesthetic awareness, and neuromuscular ability. The test is named for the leg, which is placed on the wall (Patient is lying on their left side with right foot placed on the wall – “Right” Hruska Abduction Lift Test).
Position
Patient sidelying with upper leg extended and aligned with hip and shoulder.
Adjust position of knees to wall, so that top knee is above the level of the ipsilateral shoulder.
Lower leg is flexed with lower toes positioned on the wall directly under the top foot and placed on 4 to 6” bolster.
Top palm should be placed flat on surface in front of chest and upper hand under head.
Mechanics (Discontinue test at the step the patient is unable to perform)
Step 1: ask patient to press bottom toes into wall to stabilize pelvis
Step 2: instruct patient to press bottom hip into the surface to engage lower abs and lower adductors
Step 3: ask patient to turn and raise bottom knee up or inwardly using lower ischiocondylar adductor and anterior gluteus medius, without moving top hip backwards.
Step 4: turn top heel up or top toes down without lowering bottom knee or moving top hip forward.
Step 5: attempt to raise top leg off wall while trunk and hips are stabilized in previous positions.
Grading Criteria:
LEVEL 0
Inability to position top leg in alignment with top shoulder and hip and with top knee above top shoulder without experiencing top hip impingement, sacral iliac pain or low back pain.
Malaligned pelvis and poor integration of adductors, abductors and FA rotators in frontal plane.

LEVEL 1
Ability to push bottom hip into surface.
Inability reflects weakness in bottom internal oblique and transverse abdominis or bottom quadratus lumborum or top external obliques.

LEVEL 2
Ability to raise or turn “in” bottom knee without moving top pelvis backwards.
Inability reflects poor strength or kinesthetic awareness of ischiocondylar adductor or anterior gluteus medius; or lax iliofemoral – pubofemoral ligament.

LEVEL 3
Ability to rotate top extremity inward (FA IR) without moving top pelvis forward.
Inability reflects poor strength or kinesthetic awareness of ipsilateral gluteus minimus and anterior gluteus medius, or impingement of medial femoral head on anterior medial cotyloid labral rim secondary to forward, anteriorly rotated contralateral pelvis.

LEVEL 4
Ability to raise top leg completely off the wall and hold without using lateral trunk muscle.
Inability reflects poor integration between contralateral hip adductors, and ipsilateral hip abductor (gluteus medius).

LEVEL 5
Ability to move correctly abducted top lower extremity into extension without extending low back or flexing knee or rotating leg externally (FA ER).
Inability reflects inability to extend leg with gluteus maximus during concomitant abduction and FA stabilization provided by adductors (IR’s) and anterior gluteus medius and TFL.

These references are attached below as PDF files. After clicking on them, you may have to “Allow Add On” if it pops up an error message at the top of the internet browser. You also may need to download a free version of PDF software, allowing you to view the articles below. Please contact us if you continue to have difficulty accessing the articles below.
Hruska, R. Pelvic stability influences lower extremity kinematics. Biomechanics. June 1998.
Dowling R, Hruska R. Hamstring injuries require triplanar assessment. Biomechanics, Feb 2003.
Licensed Physical Therapists and PT Assistants
Licensed Occupational Therapists and OT Assistants (Classification Codes)
Certified Athletic Trainers
Certified Strength & Conditioning Coaches
Certified Personal Trainers
Licensed Massage Therapists
Other Healthcare and Fitness Professionals
PRI welcomes any licensed healthcare or certified fitness professional to attend our courses. You may be asked to submit your license to practice as a healthcare professional or qualified fitness or strength coach certification (though an organization that is recognized in the United States) to attend PRI courses. Students studying to become a healthcare or fitness professional at an accredited universtity are encouraged to enroll, and may be asked to provide enrollment status and program/degree information. If you have questions about whether you are eligible to complete PRI courses, please contact us. Attendees are responsible for following their state statutes regulating their professional practice. A certificate will be awarded to attendees upon completion of this course or any of the other PRI courses.
Accessible Learning Environments
All participants in Postural Restoration Institute™ (PRI) continuing education courses are entitled to an accessible, accommodating, and supportive teaching and learning environment. Participants have the right to request accommodations and the responsibility to provide disability documentation that supports those requests. PRI has the right to establish eligibility guidelines in accordance with both law and policy regarding disability and provide those accommodations that appropriately provide equal access to the programs and activities it sponsors.
A Certificate of Completion is awarded to attendees upon the successful completion of this course. Before attending a course, please verify CEU acceptance with your profession’s regulating body.
Physical Therapists and PT Assistants
In the states where PRI is sponsoring courses and where approval through state American Physical Therapy Association (APTA) or licensing agencies is required, PRI will apply for approval for CEUs for Physical Therapists and Physical Therapist Assistants.
Occupational Therapists and OT Assistants
PRI is no longer recognized as an Approved Provider through the American Occupational Therapy Association (AOTA). Many states do not require any sort of pre-approval process. And of the ones that do, most state licensure boards allow self-submission of CE programs. Please check with your state licensure board to determine if you will be able to submit PRI courses for CE hours.
Chiropractors
In the states where PRI is sponsoring courses and where approval through state licensing agencies is required, PRI will look into applying for CEUs for Chiropractors (upon request). Requests must be made at least 90 days prior to the course date.
Athletic Trainers & Athletic Therapists

The Postural Restoration Institute (BOC AP# P2376) is approved by the Board of Certification, Inc. to provide continuing education to Certified Athletic Trainers. This program is eligible for a maximum of 16 Category A hours/CEUs. ATs should claim only those hours actually spent in the educational program.
![]()
The Postural Restoration Institute is approved as a CATA Accredited Provider, which enables the provider to offer courses to CATA members as pre-approved for members to earn continuing education units (CEUs). CATA CEUs are assigned to a course based on the following equation: Course contact hours x 0.4 = CATA CEUs. This home study course awards 6.4 CATA CEUs.
Strength and Conditioning Coaches

This course is approved by the Collegiate Strength and Conditioning Coaches Association (CSCCa) for 7.5 CEU’s.
Other Healthcare and Fitness Professionals
PRI Welcomes any interested healthcare or fitness professional to attend our courses. Attendees are responsible for following their state statues regulating their professional practice as they integrate interdisciplinary PRI concepts.
PRI reserves the right to cancel and refund a course attendee’s registration if any concerns arise regarding the course attendee’s qualifications as a healthcare or fitness professional, copyright infringement, or any other illegal activity involving PRI copyrighted materials. International attendees may be required to review and sign a Copyright and Intellectual Property Recognition and Disclosure Contract prior to receiving access to course materials.
Learned a ton and started to apply it right away! | October 2022
The course was everything that I expected it to be, and gave me a greater appreciation for human movement | July 2022
Better than anything I’ve learned in 20+ years! | May 2022
Absolutely amazing content! | April 2022
Phenomenal. Craving the next class already. | February 2022
Fantastic, Inspirational, Enjoyable. Thank you so much as always!!! | December 2021
A great course that exceeded my expectations. | December 2021
Absolutely incredible. | September 2021
UNREAL. Thank you! | July 2021
Fundamentally a gamechanger in our healthcare system. Buy a ticket today – it’s a heck of a ride!!! | July 2021
Thank you for creating such a thorough course manual. I appreciate being able to use the exercises and pictures for patients. |September 2020
I can’t tell you how excited I am by the work that you’ve done (are doing), bringing together concepts and techniques from various disciplines, and building a unique and incredibly insightful approach to physical therapy examination, evaluation and treatment. I realize that your work (as all of our work) is built on the shoulders of others, and I am not prone to hyperbole, nor have I ever had a hero; still, I am awed by the genius of your constructions. I am reeling a bit from all of the information I have received in taking 3 of PRIs courses in the last month, but everything I have learned has resonated strongly. There are many patients who I haven’t been able to help, many more who I could never to to 100%, and I’ve always been very away that I was missing something. Though I have treated very few patients with the PRI approach thus far, I am convinced that this is the missing link.
I am a bit of a continuing ed junkie, have taken many hundreds of hours of courses (most of them excellent) and am in the process of completing my DPT degree, but I have never encountered coursework that was this inspiring. It seems that you are grossly under-appreciated in the physical therapy world and I just want to thank you for all you have done and all you continue to do. | St. Louis, Missouri, February 2013
Course
You will receive an email within 24 hours after purchasing the home study with instructions to login and begin your home study online. (*Please note that you must order before 3pm CST on Friday to receive your online access information before the weekend. If you order the home study after 3pm on Friday, you will receive your online access information on Monday). You will receive all materials online including the videos and course manual (which you will be able to download and print). You will also complete the post-test and course evaluation form online. You will need high speed internet in order to watch the videos (the videos are NOT downloadable). Once you have been emailed your online access information, you will have 21 days to complete the course online before your access to the course materials will expire.
You will receive a Certificate of Completion by email if post-examination test is passed (miss 8 or fewer) and course evaluation summary is completed.
Online/Digital Format – Each registrant will receive online access to the approximately 15 hours of course video content, as well as access to download and print the entire course manual (printing the manual is recommended). The post-test and course evaluation form will also be completed online. You will have 21 days to complete the course material, before your online access expires.
Special Needs Requests
If you have a disability and require accommodation in order to fully participate in this course, please contact us prior to purchasing any online home study course so that arrangements can be made.
Cancellation and Refund Policy
To cancel your registration, please call as soon as possible for a full refund. Cancellations and refunds will not be accepted once the course registrant has set up their online username/password.
Those who have earned the designation of Postural Restoration Certified (PRC) or Postural Restoration Trained (PRT) are eligible for a 50% discount. Students are eligible for a 25% discount.
If you have taken the live course in the past 12 months you are eligible for 50% off the regular price.
Copyright © 2008 - 2024 Postural Restoration Institute® (PRI). All rights reserved.