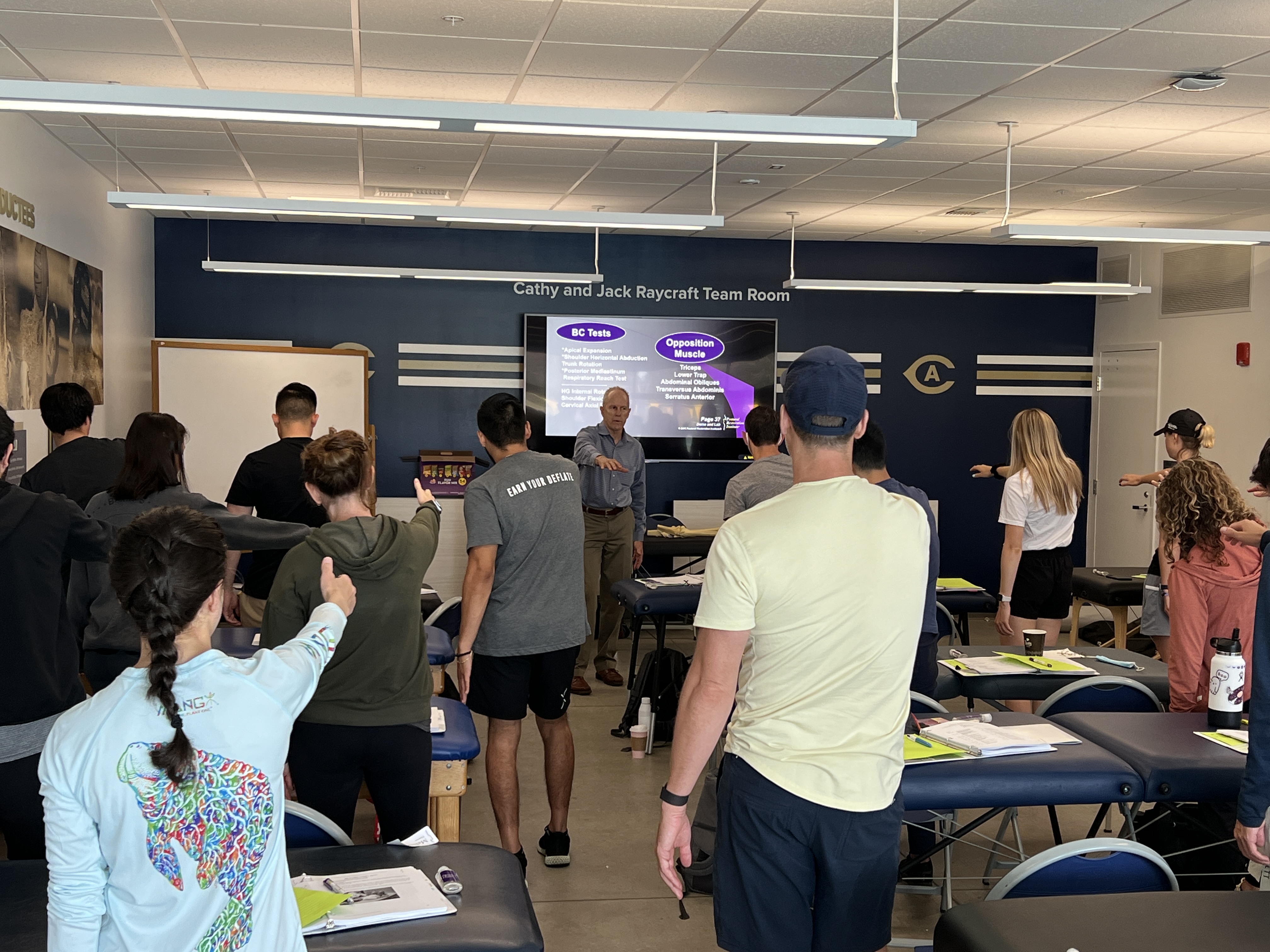
It is not often that almost an entire group of course attendees are not only new to PRI but nearly the entire group is new to Postural Respiration. In addition, a large number of the course attendees where affiliated with the host site and staff at the University of California at Davis sports medicine department. The combination of new course attendees and the cohesive group from UC Davis made for an entire group experience that this faculty member will remember for a long time!
Respiration is the heart and soul of PRI and how we manage pressure sense neurologically is a post graduate subject that this group new to PRI grasped immediately. For new students there where questions through out the weekend that re-enforced all of the concepts of this course and the basics of PRI. Everyone of us can remember their first course and how daunting a "paradigm shift" can be. This group of students shared this shift in a step-by-step journey into the wonders of this course where it appeared that all were pulled along by each other in this endeavor to learn. Was it and is it always daunting for new students to be introduced to PRI for the first time or to a new course? Yes but the energy and attention held throughout the weekend was impressive to say the least! And, the UC Davis team now can share, practice and grow in their PRI journey together to provide care to their athletes and each other. I look forward to returning to Davis one day and to see this community of professionals grow in taking all of the primary courses and moving on to secondary and tertiary courses in the future. Thank you much to Melissa, Sammatha, Doug, Lisa and the entire UC Davis Sports Medicine Team for hosting.
Po kilkuletniej przerwie, ponownie mamy przyjemność zaprosić Państwa na kurs PRI w Polsce. W ramach Kompleksowego Kursu, w Polsce odbędzie się pełen podstawowy kurs metody Postural Restoration Institute. Co warte zaznaczenia, odbędzie się on w innowacyjnej, hybrydowej formie, dzięki czemu jego uczestnicy zyskają dwa dodatkowe dni nabywania praktycznej wiedzy oraz dodatkowe narzędzia ułatwiające zrozumienie i wdrożenie tej koncepcji terapeutycznej do pracy.
Co wyróżnia tę formę prowadzenia kursów? Poza trzema podstawowymi modułami kursu PRI, zawiera ona dodatkowy moduł, podczas którego przez dwa dni poruszane będą praktyczne metody pracy zgodnie z wytycznymi Postural Restoration Institute. Na uwagę zasługuje także hybrydowa forma prowadzenia szkolenia. Moduł I i IV odbywać się będą stacjonarnie, zaś II i III w pełni zdalnie. Co więcej, pomiędzy modułami odbywać będą się webinary, na których powtarzana będzie zdobyta wiedza, a uczestnicy będą mogli rozwiać wątpliwości dotyczące praktycznych wdrożeń metody. Podsumowując, kurs będzie realizowany w następującym schemacie:
4-6.11.2022: I Moduł: Oddychanie Posturalne – Zintegrowane Podejście do Postępowania Leczniczego i Patomechanika Wzorców Kompleksu Piersiowo-Brzusznego
3-dniowy kurs stacjonarny w Warszawie
I Webinar: Krótkie powtórzenie modułu I oraz praktyczne Q&A
II Webinar: Krótkie powtórzenie modułu II oraz praktyczne Q&A
13-14.05.2023: III Moduł: Odbudowa Miednicy – Patomechanika Wzorców „Łonowo-Krzyżowych” – Zintegrowane Podejście do Postępowania Leczniczego
2-dniowy kurs online
III Webinar: Krótkie powtórzenie modułu III oraz praktyczne Q&A
17-18.06.2023: IV Moduł: Manualne i niemanualne techniki inhibicji i facylitacji. Część praktyczna rozszerzająca treści z modułów II i III.
2-dniowy kurs stacjonarny w Warszawie
Koszt każdego modułu wraz z webinarem powtórkowym to 2199zł. Szczegółowy program oraz informacje organizacyjne znajdują się na stronie https://inspirowaniruchem.pl/kurs-pri/
Uczestnicy szkolenia po każdym module otrzymają certyfikat Postural Restoration Institute.
I always like travelling back to the Northeast especially when I get a chance to teach in Boston. This trip was extra special as I was able to bring my girls and husband with me for the weekend and a little extended getaway for me! The girls have grown up with PRI and it is fun to watch them (not medical) be able to identify a pattern in the way someone walks!
I had the pleasure of mentoring one of our new faculty members Jason Miller. Jason and I taught the course together. Even though the Celtics did not win on Sunday night, I’d say his performance was a slam dunk. This class was not much different demographically speaking from most Myokinematic of the Hip and Pelvis that I have taught over the years. Most attendees were taking their first course and some had taken multiple. The cool part was everyone had some exposure to the science and were eager to learn the why behind what we were doing with the PRI methods. We explored patterns, how it changed position and could result in pain or decreased performance. Speaking of performance, I was also fortunate to have Eric Menchi as a lab assist. Eric has been around PRI for awhile and was able to provide insight as to how he applies PRI science with his personal training clients. Jae from Northeatern also spoke to the application of the Northeastern Athletes in both the training room and how they integrate with the strength and conditioning staff.
Let me say this to those that are struggling. The struggle is real and PRI is not an easy science. It makes you think long and hard about what your patient is doing and how they are compensating whether that is good or bad. It is our mission to help our patients clients and athletes to better movement with less pain and of course better function! This course provides the new learner a gateway to apply and progress following algorithms that have stood the test of time. It was pleasure to mentor Jason and teach a room full of enthusiatic learners the science of PRI and yes, I did my best to stay on topic with the hip!
The PRI Credentialing Scholarship application deadline is just a few days away. If you are interested in applying, please make sure your essay is emailed to Jennifer Platt by June 15th!
This $2000 full scholarship is available to candidates who may otherwise be dissuaded from applying for PRC or PRT credentialing solely by their current financial circumstances. To apply, please submit a scholarship essay sharing your story of how you got to where you are (i.e. how you became interested in PRI, do you have any mentors or colleagues supporting you on this education journey, etc.), your current professional and financial situation, what PRI credentialing means to you, and why you feel you are deserving of the scholarship.
All essays will be reviewed by the PRI Board of Directors, and the scholarship recipient will be notified by July 15th. If the recipient of the $2000 full scholarship does not accept the scholarship and complete the credentialing application and testing within the year, the scholarship will be awarded to an alternate. Depending on the number of applications each year, the Board of Directors may choose to select more than one scholarship recipient.
If you have any questions with the PRI Credentialing Scholarship, or any questions with the PRC or PRT credentialing process in general, please contact me!
My name is Daniel Bek. I live in NYC and intern at NYDNR. They are looking for a physical therapist in the tri state area that is looking to work part time or full time from 4-8pm monday-friday. If any one is intrested in this positon please email iuliia.andrushchenko@gmail.com.
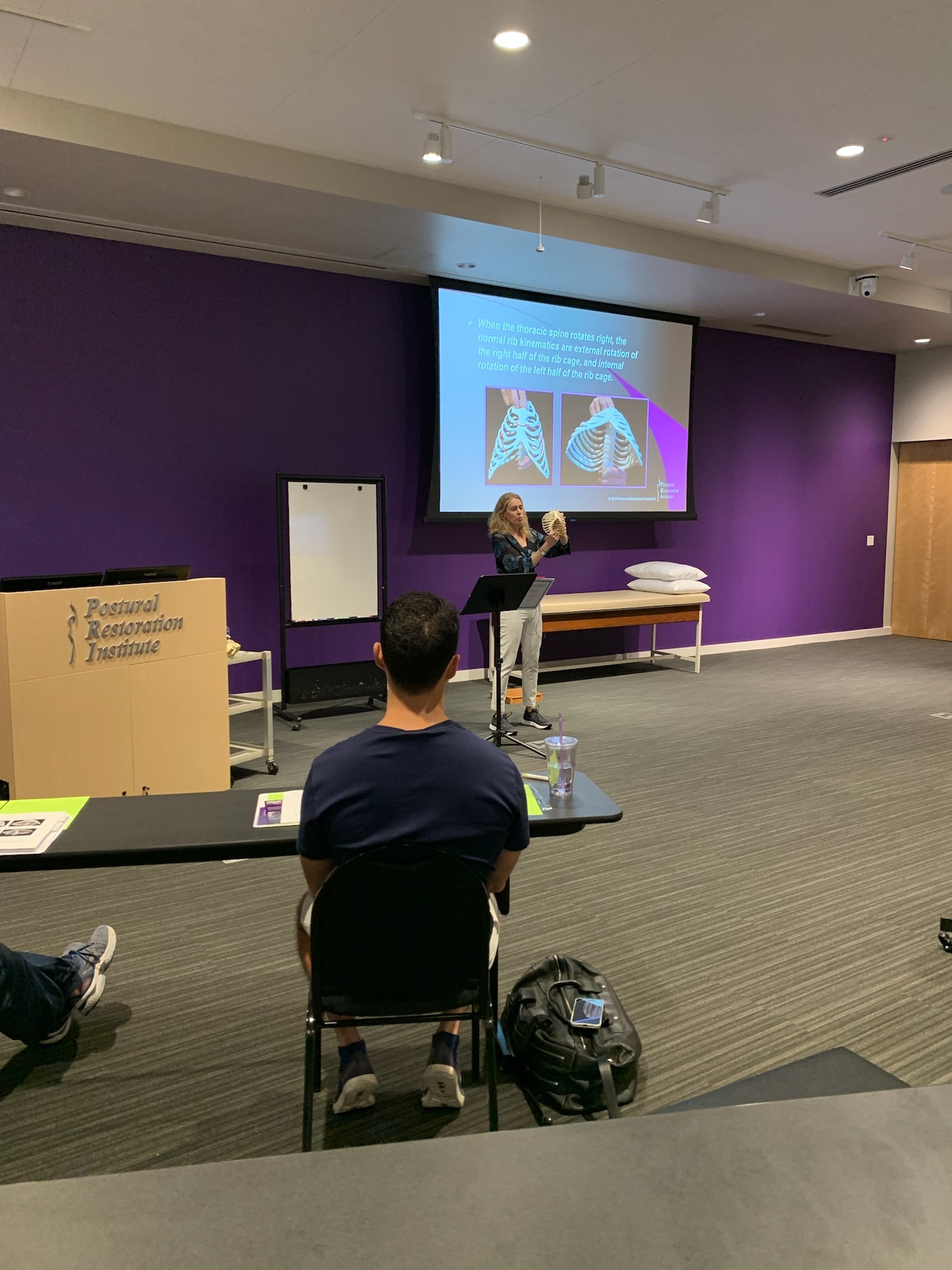
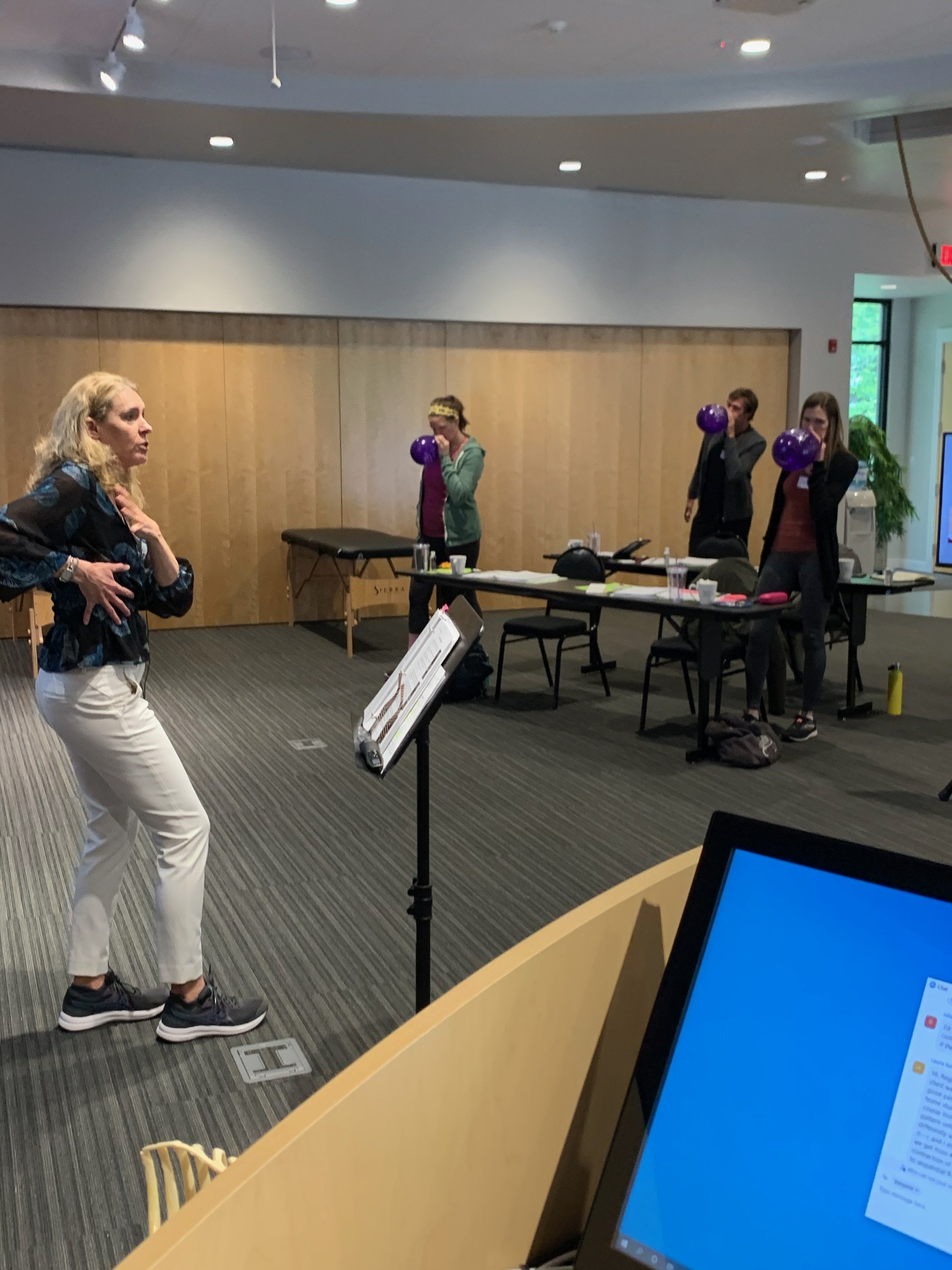
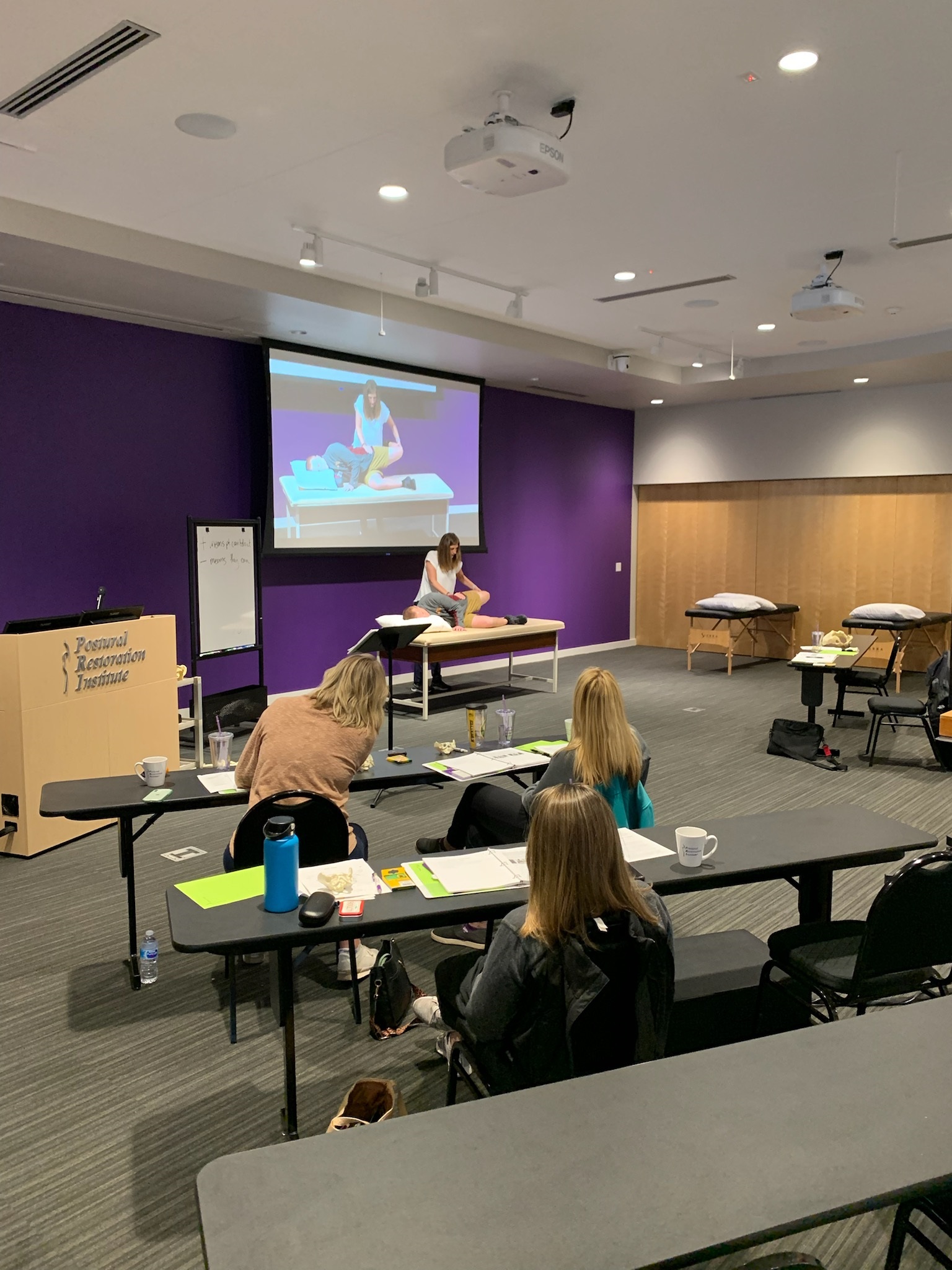
I really enjoyed presenting Postural Respiration at the very place that PRI began – Lincoln, NE – to a hybrid group of enthusiastic and inquisitive in-person and virtual attendees.
We spent the weekend learning about the influences of the left AIC, right BC, and bilateral PEC patterned overactivity on hemi-chest compression, air flow, and movement. Our most primal movement pattern, respiration, is directly reflected in how we move our bodies in space. The quality, efficiency, fluidity of our walking is directly impacted by where air is directed in the chambers of our thorax. The numerous videos and photos, presented throughout the weekend, provided stark examples of the deleterious effects of patterned respiratory mechanics on upright posture and movement.
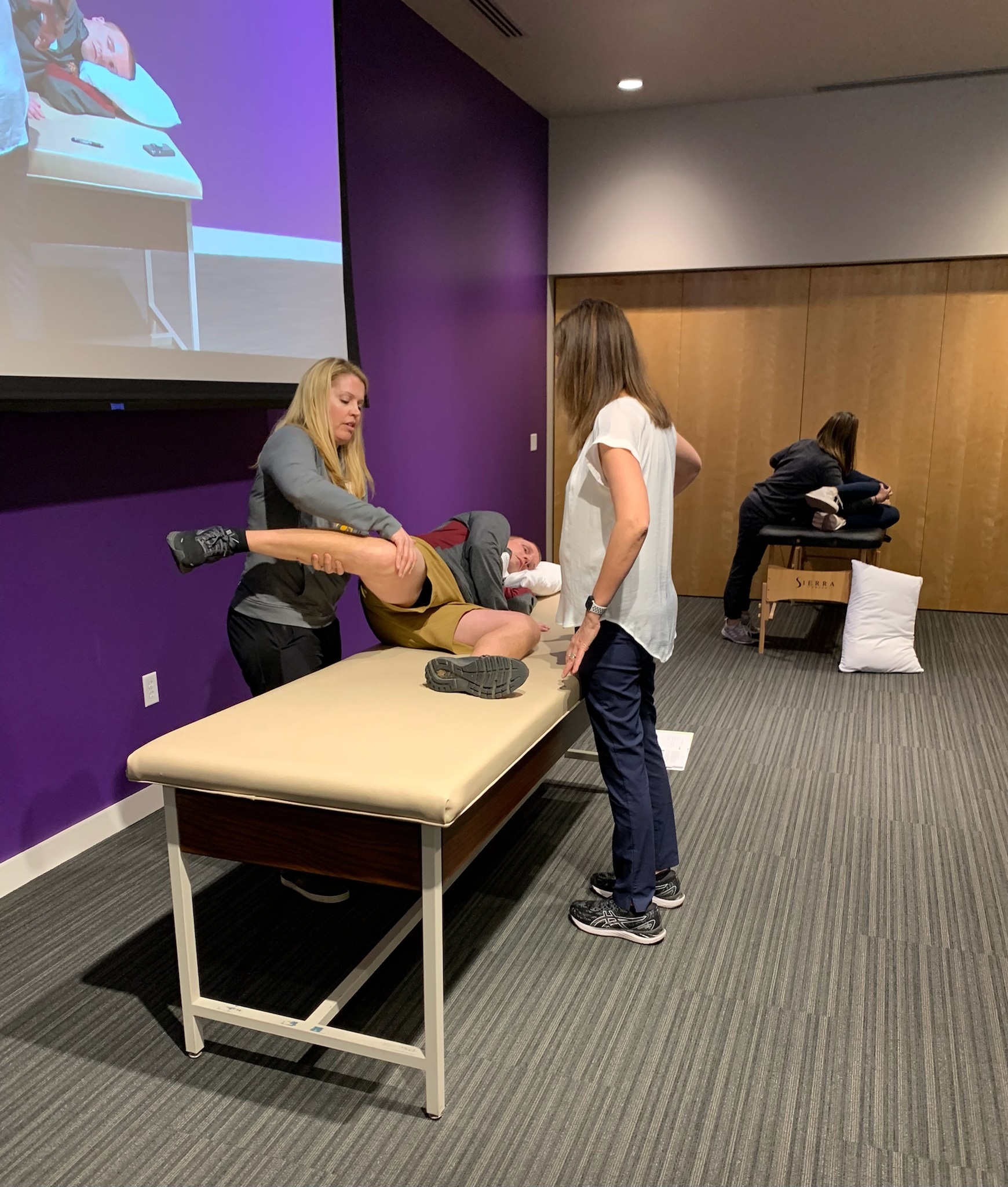
Through lab breakouts, the in-person attendees helped me talk through and demonstrate how to determine if, and how much, a person is being driven by polyarticular muscle overactivity that prevents proper compression and decompression of our systems for healthy movement and physiology.
This being Lincoln, NE, and not Providence, RI, balloons were back in business, allowing attendees on both sides of the screen to experience eccentric and concentric abdominal contraction and air flow into previously compressed regions of the thorax.
We discussed how the ability of the right 1st rib to move reciprocally is key to enabling the remaining ribs to reciprocally move. Its ability to raise and lower for compression/decompression of the apical chest wall is compromised with overactive scalenes that encourages the subclavius to join the party. With this disruption in hemi-rib uniform movement at rest, we become stuck in a respiratory state of twist that an individual doesn’t know how to get out of. Hemi-rib uniform movement at rest is a prerequisite for calming the nervous system, so that we can truly rest at night.
Thank you for the many questions to clarify concepts for all attendees. I think I speak for everyone when I say the additional insights that many of you provided, especially in response to the non-manual techniques, were helpful and appreciated. Finally, a big thank you to RJ Hruska for deftly handling the A-V while answering questions and keeping this instructor hydrated and on schedule!
The skepticism I had 42 years ago, as I graduated from a Physical Therapy program, regarding models of education and health care practice remains with me today. I pursued a Masters in Public Administration to learn how cities, administrations, etc. collaborate and communicate for the benefit of the inhabitant. I learned a lot about business, how the top of the pyramid develops and what paradigms, courageously were successfully encountered and embraced.
When I read the forward of Dr. James Calson’s book ‘ Physiologic Occlusion’ I remember thinking about his comments about “societies” and how much I agreed with his philosophies. He wrote, “Dental societies, associations, foundations, and academies sponsor journals and other publications for the dissemination of scientific articles to the dental community. It is interesting to me that all are accompanied by length bibliographies. I wonder who wrote the first dental paper and what the bibliography included. Sometimes it seems that authors are compelled to have large bibliographies to satisfy the critics and skeptics of new and compelling information. Could it be that they are afraid to ‘stand alone’? Afraid that they won’t be accepted on the merits of their own work? Afraid to say anything that is not based upon the work of others who are already accepted and respected in the dental community? I may be wrong in that assumption, but I don’t think so. Copernicus, Einstein, Columbus, Leonardo da Vinci, and many others challenged the current thinking of their age, and today we live with the benefits of their Paradigm Shift.”
Having the opportunity to share and discuss my thinking regarding the Stomatognathic System with someone whom I have always considered a silent mentor, for so many reasons, is truly an honor. This opportunity, probably will not come again in our lifetimes, and for that reason alone, I am so grateful. Dr. Carlson is a giant when it comes to education and paradigm shifts.
“Do not conform to the pattern of this world, but be transformed by the renewing of your mind. Then you will be able to test and approve what God’s will is – His good, pleasing, and perfect will.” (Romans 12:2)
– Ron Hruska
Someone once said, “you don’t know what you don’t know.” So, it is with those of us who are “students” including me. For almost 30 years I have been traveling from home, both here and abroad, to many countries around the earth to share what I have learned to be true. In so doing, I have met several hundreds of people most of whom have been kind and hospitable including everyone at PRI with Ron, Jason, Jennifer, and RJ being tops on my list.
I was also most impressed by the level of the content of all the information that Ron and Jason presented.
My “world of dentistry” would be wise to listen to the knowledge and information that is being presented in all of your programs.
That might just make a difference between “knowing and guessing.”
Science is all about expanding the realm of human perception and human sense. Life is both. This tertiary course allows me to discuss how a change in perception and sense of the visuo-spatial cortex, hemi-chest compression, upper extremity reciprocation and lower extremity alternation of mass management can influence dominance or patterned design outcomes. A change in perception related to any one of these components, changes perception associated with the other three. This predominant component patterning, precedes our cortical and associated physical, physiologic and psychologic dominance in moving ourselves forward. I asked two individuals who attended this course to provide some honest, visceral feedback about the material that relates to the assessment and treatment of functional cortical dominance. Thank you Andrew Hauser ATC, CSCS, RSCC, PRT and Robert George DC, PRC for the following insights.
"I feel like I could write quite a bit about this subject as everything I felt like I learned in Vision& conversations from both you (Ron) & Heidi all came flooding back, and then some. It integrated all of it, and I appreciated how good of a job you did regarding bringing up what was backed by research. Simple, complex and everything in between. It’s tertiary for a reason, there is no doubt, but it felt like I could finally share what I had learned from you that others hadn’t yet experienced. It put it into words. I’m sure each course will be different, yet the golden thread will remain.
Where to begin?! The FLM course brought concepts from the previous vision courses, advanced integration and the primary courses and truly integrated them into what is driving the show on a daily basis. Being able to take all the phases of gait and break them down through our visual processes, hemi-chest airflow, upward limb alternation and how the lower half is responding & supporting these components of forward locomotor movement was a revelation. Understanding the biased-cortical / hemispheric "need for speed" and our abilities, as practitioners, to slow everything down may have turned this into a course on psychology, that wasn’t a course on psychology. I think they just took the lid off of Pandora’s box." – Andrew Hauser
"Last weekend Ron presented FLM and for this faculty member it was an experience that opened the door wider to PRI tertiary principles. Integrating Hruska hemispheric components of vision, hemi-chest wall airflow and upper limb alternation first, then considering lower limb alternation, really cemented the basics of forward locomotor movement. The course also opened the door to more questions for me especially when Ron was talking about the “trombone” effect of near and far vision for FLM.
I called Ron after this course today with not only questions but a realization that this last weekend so many light bulbs went on in my head that opened a gateway to somatosensory topics. I must confess when I took the vision course several years ago, I didn’t understand much after words! I was just learning to teach the basic mechanics of primary course work and was overwhelmed by what seemed to be a really complex subject. After this past weekend, not only did the vision course make more sense, but tertiary course concepts from Cranial Resolution and Occlusal Cervical Restoration became more clear as the sensory and motor components of coordinated and balanced movement were revealed.
One of my questions for Ron was regarding Functional Cortical Dominance. In our talk today, Ron was discriminating between cortical dominance as well as individual pre-dominance developed over time. In Postural Respiration, we present the very basics of the left half of brain contributing to right sided dominance. But the discussion is much more complex including what we see, hear, feel, sense from the ground, temperature, where sound is coming from and the visual kinesthetic sense of movement and flow of things going past us. This is a short list of sensory input in addition to a psychological component of how we respond to the mystery of being alive for a sense of well being!
In a recent walk I had in nature with Ron and Robin, the topic of discussion was the very human hunger and need of having a sensual experience in nature for our mental and emotional wellbeing. Filling our senses the sight of waterfalls, rivers flowing into pristine lakes, seeing the varieties of color, wildlife and trees all fill a need for a sensual experience. Ancient natural sound that we have heard as humans for thousands of years like the sound of wind in tall trees, flowing water falls, a thunderstorm and the sound of wildlife including birds and a coyote call are all in our DNA. The mille-second processing of natural sounds orient us in time and space and even feeling the wind on one side of our face gives us a sense of direction and orientation as well. Becoming conscious of and feeding all of our senses we all hunger for but have become unconscious or disconnected from in a converged modern world. These somatosensory experiences expand our awareness, feed our mind and emotions beauty and inspiration and allow for the joy and freedom of movement that is rare in a paved over, domesticated and confined modern experience we just assume is “life”.
Sensory processing though our five senses is a complex, multilayered experience affecting all parts of our brain all at once with horizontal and vertical movement, flow and forward motion and a mental and emotional response that is processed unconsciously and consciously instantaneously.
Ron asked be for a brief recap of my brief discussion today and as I see it as movement specialists in PRI, expanding and becoming more conscious of our own sensual acuity with the purpose of understanding not just human movement, but providing a path to more sensory awareness, internal mental and emotional fulfillment and well being for our patients and ourselves is a worthy endeavor." – Skip George
I recently had another great oppurtonity to teach Pelvis Restoration at the home of the Postural Restoration Institute. This was the third Live Stream course that I have instructed and it was truly one of the best! I had a smaller live group of 6 on site attendees and over 20 Live Zoom participatents. I did my best to stay focused on the introductory concepts, tests and treatments for pateints suffering from Pelvis related dysfunctions. I enjoyed the discussions regarding patterns, positions and PRI as it relates to frontal plane control of the Pelvis. I really enjoy discussing Pelvis Respiration as it can benefit so many patients and give PRI therapists a greater understanding of how the thorax, inlet and outlets all integrate to stabilize our pateints. Thanks to RJ for being my Mystro this weekend. He always takes good care of me and our students.
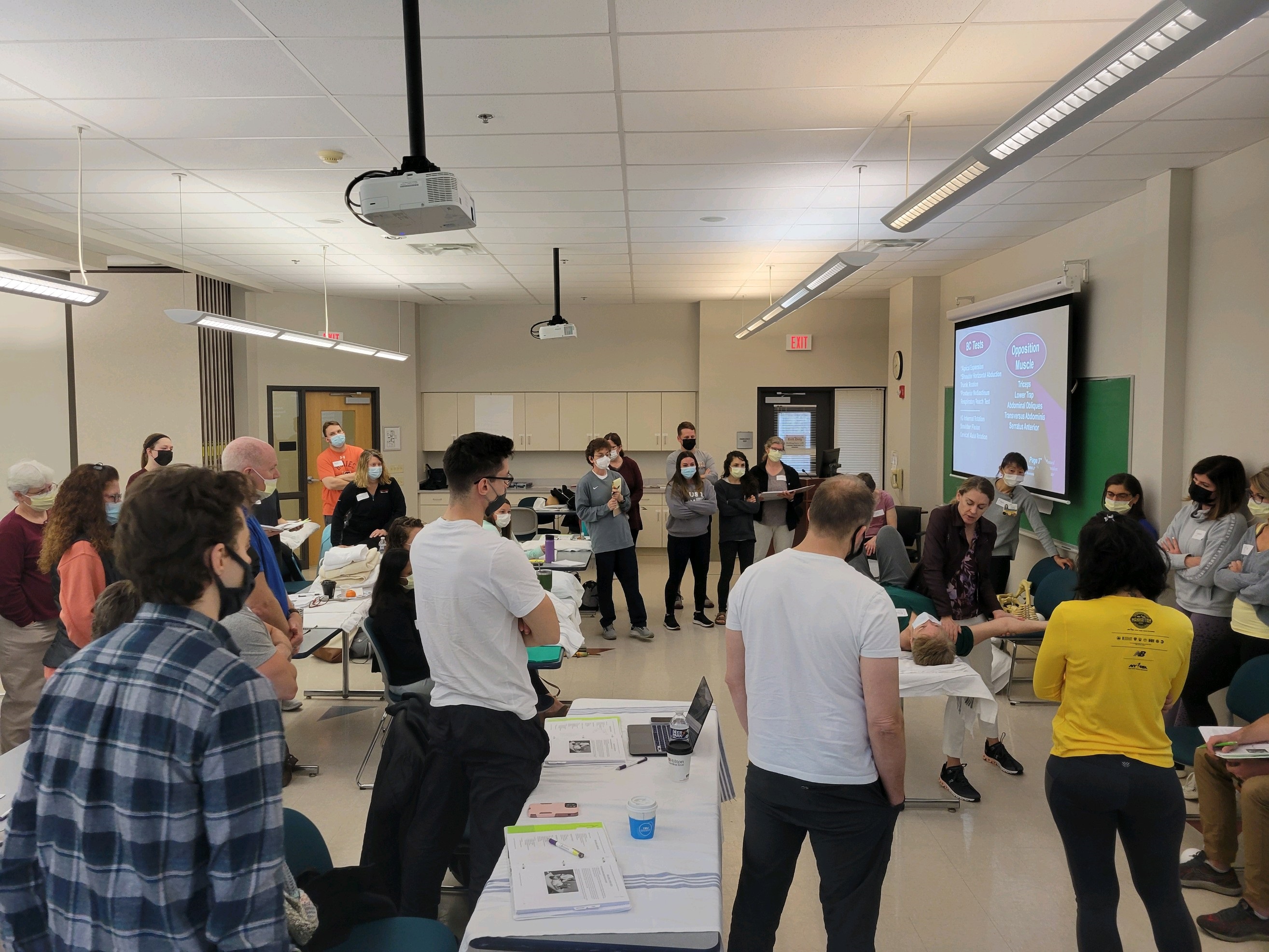
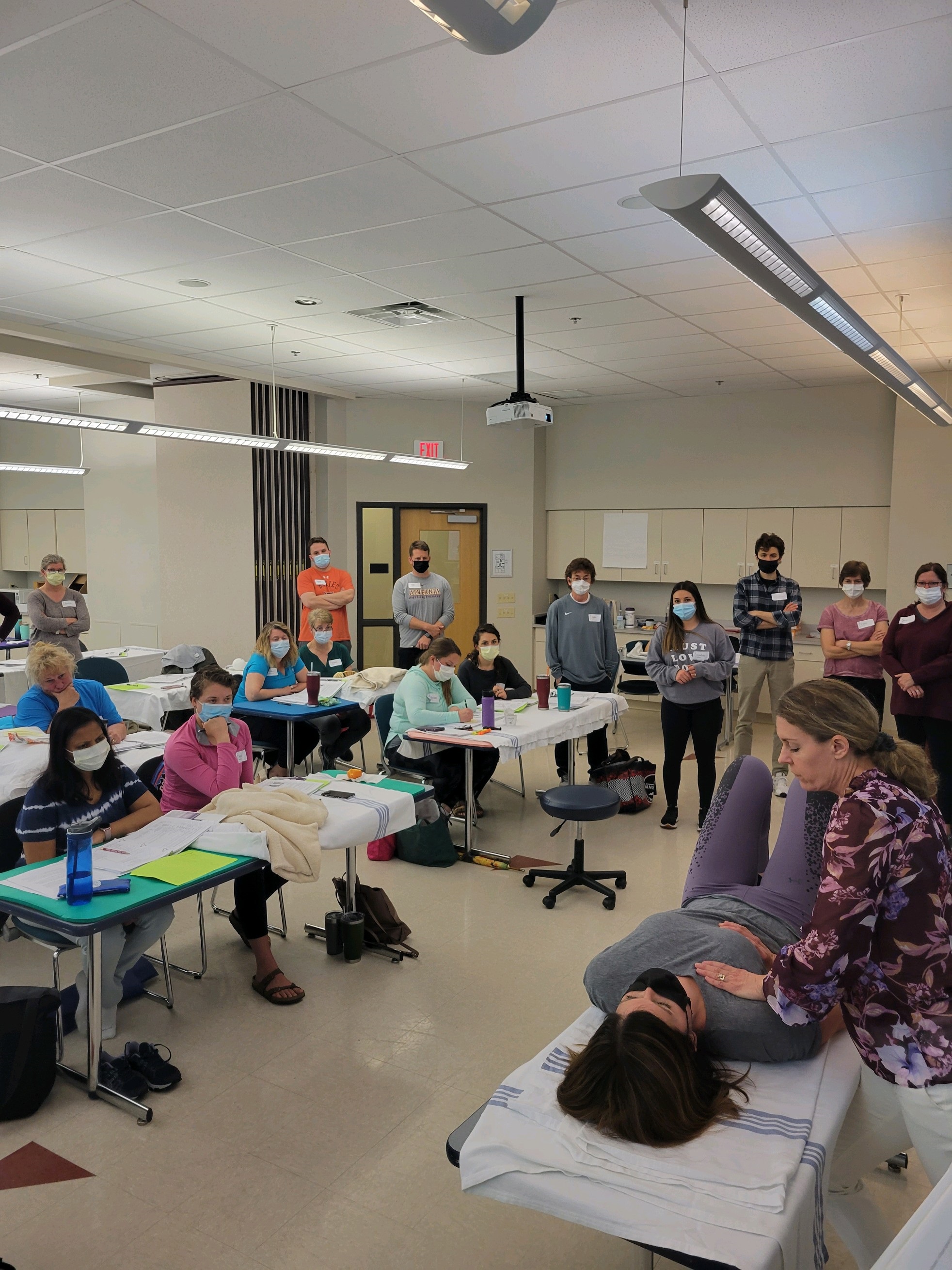
The clinicians of Lancaster General Hospital are pros at hosting PRI courses. Last weekend’s Postural Respiration course was their seventh. This instructor had moments of déjà vu, since LGH was the location of the first PRI course I attended, back in 2007. Two participants, Deborah Schrodi, PT, and Cathy Ingram, PT, were also in attendance at that very course 15 years ago! The surrounding Amish community, who eschew automation, provided an interesting contrast to our modern way of life and its epidemics of myopia, asthma, and loss of movement variability. These modern ills can be traced, by-and-large, to technological “advancements”.
Underscoring the Institute’s interdisciplinary mindset, the class was comprised of a mix of clinicians, including physical therapists, physical therapy assistants, athletic trainers, massage therapists, and personal trainers. Many were new to the science, while others had multiple PRI courses under their belt.
The Institute continually works to update course material, adding research articles and patient photos and videos to illustrate and support course concepts. Our left and right hemi-diaphragms are different in size and have differences in abdominal support. This “static asymmetry” creates a teeter-totter effect within our body, keeping us reflexively alive and providing a starting point from which to move. When this teeter-totter situation reaches a tipping point, we have only a “totter”. The right side remains pinned-down, grounded, and compressed. The left side is held aloft, remaining ungrounded and decompressed. We cannot thrive in this state.
Our patterned, maladaptive hemi-diaphragm position and activity has consequences on movement, physiology, and behavior. Humans require oscillating compression and decompression of our lungs and rib cage to provide movement and ensure the health of our tissues, most notably the nervous system. An outward sign of this lack of oscillation is breathing pattern dysfunction, such as belly breathing, chest wall elevation, and superior T4 syndrome, the underpinnings of many of the syndromes that we treat.
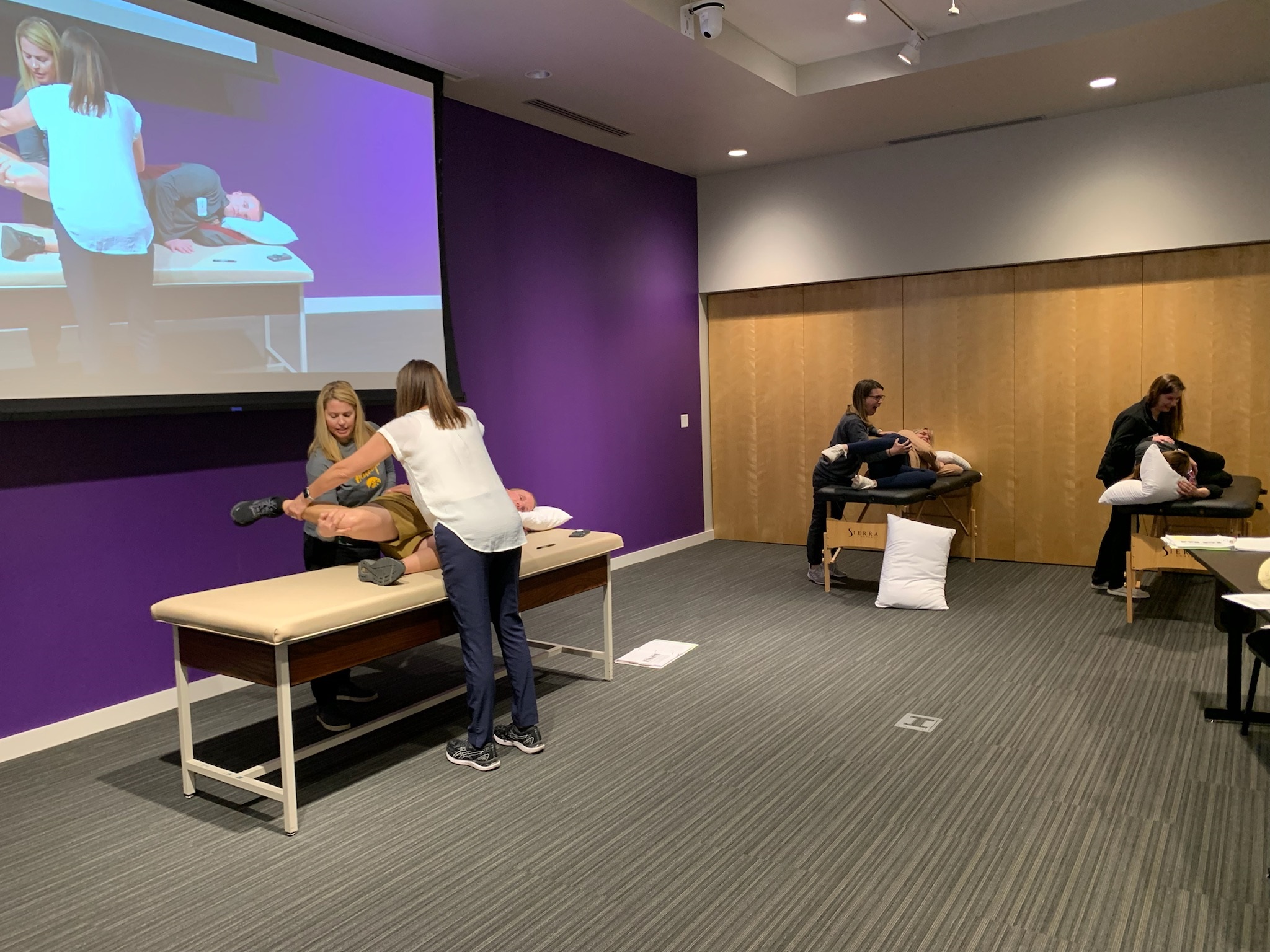
Postural Respiration is a lab-heavy, hands-on course, better taken live, if possible. Participants came away proficient in performing and interpreting PRI’s objective tests to identify overactive left IAC, right BC, and B PEC chains of muscles and the pesky superior T4 syndrome. These patterns need to be inhibited so that we can efficiently and effectively inhabit the environment around us, without deleterious effects on our neuromusculoskeletal system.
A huge shout out to Frank Mallon, DPT, PRC, owner of Renaissance Physical Therapy in near-by Philly. Your expertise and instruction on the nuances of the Institute’s non-manual and manual techniques was invaluable!
Thank you to all who asked questions and provided clinical comments, keeping the energy level high. Thank you to our models, who enhanced the learning experience: Kirsten Ditzler, DPT; Kelly Faller, PTA; Eileen Herman, PT; Isha Mody, PT; Joesph Newton-Pretko, DPT; Kyle Price, PT; Lori Shearer, PTA and Michael Polejav, PT who all helped facilitate our learning.
Thank you to the LGH clinicians for your efforts in set-up and clean-up. I appreciated the opportunity to present this material at the place where my PRI journey started.
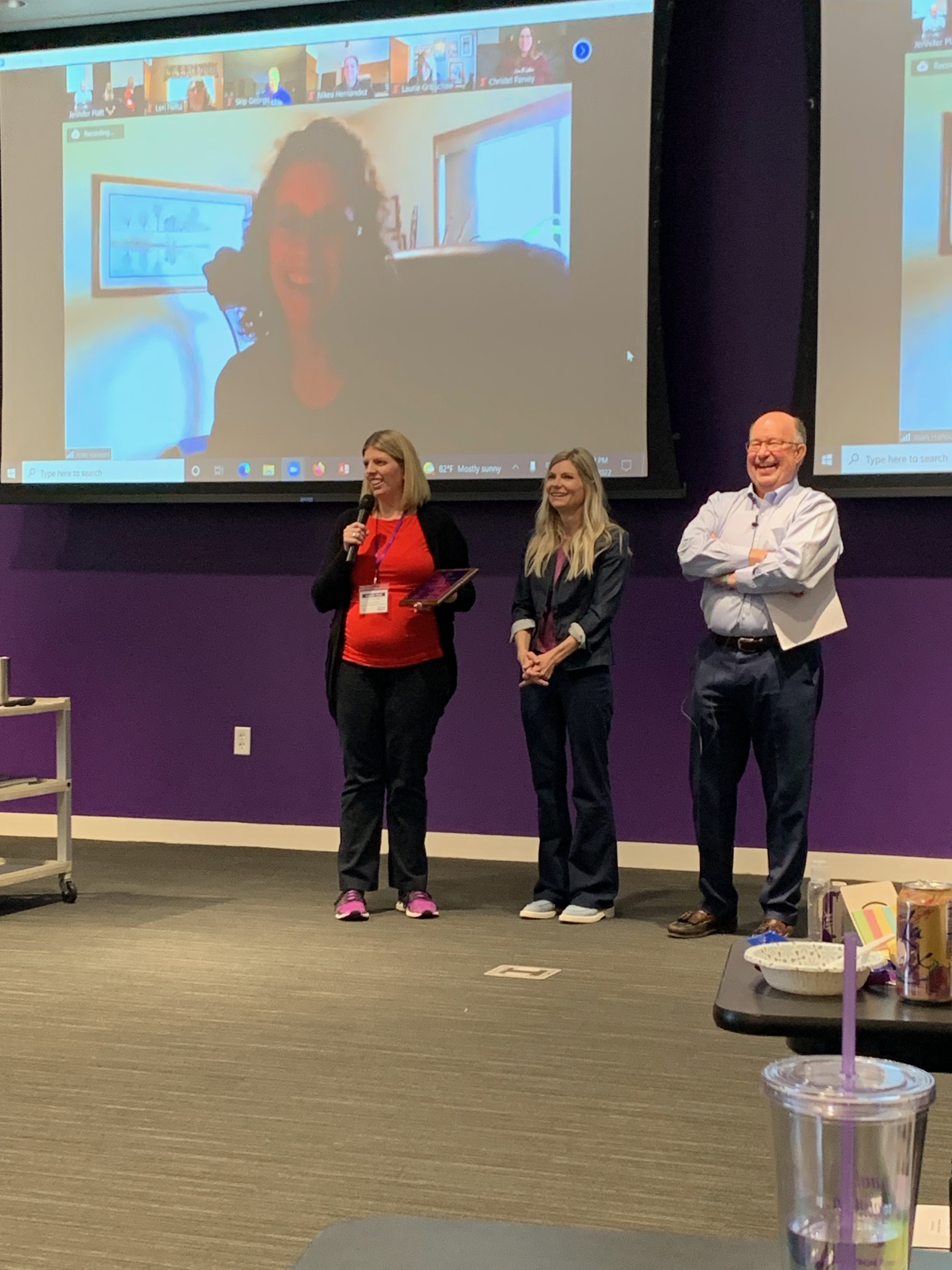
Last week, at our Annual Interdisciplinary Integration Symposium, we presented the PRI Director’s Dedication Award to two very deserving individuals who have had such a positive impact on our Institute; Joan Hanson and Robert "Skip" George. Although they were unable to join us in-person for the symposium this year, we knew we didn’t want to wait to present them with this award, and so we did so virtually, with 40 in-person attendees and approximately 90 others watching on the live stream feed. The PRI Director’s Dedication Award was established by the Board of Directors (Ron Hruska, Janie Ebmeier, Jennifer Platt and Bobbie Rappl) in 2012 to recognize individuals’ ongoing dedication to their advancement in PRI. To date, we have presented this award to 18 individuals and an award recognition plaque, which is pictured above, is displayed at the Postural Restoration Institute® in Lincoln, Nebraska, recognizing each of the PRI Directors Dedication Award recipients.
Joan Hanson is a Physical Therapist in Sioux Falls, South Dakota. Joan began her PRI journey 22 years ago, with a Protonics course, and since then has taken 32 PRI courses. She completed PRC credentialing in 2005, as part of the 2nd class to complete PRC credentialing. Joan owned an outpatient clinic, Physical Therapy Solutions in Sioux Falls, prior to merging with Sanford Health; now operating as Sanford Physical Therapy Solutions. Joan continues to make her presence felt in the PRI community, by attending courses in Lincoln on a regular basis, contributing questions and responses to peers in the PRI Google group, mentoring the colleagues at her clinic, and being an avid PRIVY fan, who regularly asks questions that prompt further PRIVY discussions. I have no doubt that Joan has watched every PRIVY, and many of them more than once. Joan is a life-long learner, and that includes merging other approaches with PRI for the best patient outcomes. She recently completed a week long Schroth training, and looks forward to integrating this approach within her practice. We feel like this award is long overdue, and we were so honored to present the PRI Directors Award to Joan Hanson.
Robert "Skip" George is a Chiropractor, who now resides in Logan, Utah. However, Skip spent much of his life and career in La Jolla, California, before moving to Utah this past year. He traded in surfing for weekly skiing or hiking, depending on the season in Utah. Skip took his first PRI course in 2012 and he completed PRC credentialing in 2014, becoming the first chiropractor to complete PRC credentialing. Skip was invited to begin training to teach on the PRI faculty, shortly after he completed PRC credentialing. He began teaching Postural Respiration in 2016, and Cervical Revolution in 2020. Skip is passionate about growing the science of Postural Restoration in his profession, and he has presented at numerous national, state and even international chiropractic conferences, including the American Chiropractic Board of Sports Physicians annual conference, the American Chiropractic Association Rehab Council, the American Chiropractic Association, and the German Sports Chiropractic Association, among other state conferences. Skip is presenting next month at the California Chiropractic Sports Symposium on the “Two Roles of the Diaphragm for Chiropractic Care, Rehab and Sports Performance”. Skip is a vibrant member of our faculty, who is constantly wanting to learn more, and has become a wonderful mentor as he assists others in their training to teach PRI courses. We were incredibly honored to present the PRI Directors Dedication Award to Skip George.
Congratulations to both Joan and Skip! We are so honored, humbled, and proud to have you as friends, colleagues and PRC providers representing this Institute!
The pacific northwest has been a PRI hot bed for several years. The enthusiasm for the science and clinical application of PRI is palpable. It was my honor to have the opportunity to teach a fantastic group of movement professionals in Seattle. We had five PRC’s in attendance for this newly updated I&I course.
This course is the perfect gateway to several PRI courses, including Cranial Resolution, Forward Locomotor Movement, and the Primary Non-manual Techniques Workshop. Our conversation starts with introducing the neurological learning process that the body needs in order to inhibit patterned behavior: alternating compression and decompression. This important concept is the foundation we build from as we progressed from the calcaneus to the femur and pelvis and into the scapula.
Founded in the concept of alternating compression, we were able to delve into medial and lateral hamstring relationships, as well as when and how to apply the right serratus anterior and subscapularis into a program. Along the way, the necessity of compression of talar bone and calcaneus, and management of pelvic inlets and outlets provide the necessary sense the body needs to allow the body the freedom it desires above T8.
I cannot thank the staff from Alpine Physical Therapy enough. Jeremiah Ferguson, DPT, PRC, Christopher Murphy, DPT, PRC, and Eva Bilo, DPT, were the perfect hosts. A huge shout out to their friend who was kind enough to loan us his projector for the weekend. It would have been a very different course without his generosity. My sincere thanks to the Alpine crew for all of their help.
We were fortunate to have a great mixture of seasoned PRI veterans as well as several who are relatively new to PRI. My thanks to Trevor Corrado, Jeff Fjelstul, David Shamash, and Katie Schaner for their willingness to ask questions. In addition to the Alpine staff, it was wonderful to have Erin Coomer, Zach Hawthorne, Wren McLaughlin, and Betsy Baker-Bold contribute their experience and perspective to the audience. It was helpful to have others in the audience provide their clinical validation to the topics of I&I.
Many thanks for a wonderful experience in a truly gorgeous region of the country!