There are four kinds of documentation that most of us use to change our behavior:
1) Learning oriented tutorials.
2) Goal oriented how-to guides.
3) Understanding-orientated discussions.
4) And, information-oriented reference material.
Each of these four types of documentations usually have instances within the document that refers to related information elsewhere in the same document. This is important as it forms a network structure of relations that exist between different parts of data, dictionary-internal as well as dictionary-external. If the cross-reference mechanism is well designed, visibly or technically, the reader, and in this case, the course attendee, will be able to follow each and apply ‘cross-reference’ event, to the referenced content whether the content is presented visibly or technically.
The last example, of the four listed above, enhances usability and application of content in each of the PRI Non-Manual Techniques. Documentation or description that identifies direct reference and referent sites of consistent interest; is required so documentation that indirectly implicates cross references from these and other discrete or unconsidered sites can provide content-strategies to meet the desired needs and expectations, from both the provider and the participant.
As the author of these techniques, and as the author of cross-referencing design associated with each technique, effort to ensure that location and content of the target of the cross-reference in each technique needs to be consistent, regardless of the aptness of the provider or the participant.
These opportunities to provide my reasoning behind each of the techniques, that were selected by this course’s participants, are not exceeded in any other course offered in PRI. Therefore, the guidance I offer to answer questions on the ‘why’s, ‘when’s, ‘who’s and ‘what’s regarding each technique’s reference’s, referent’s, and cross-reference’s content, is an absolute unique opportunity for both the author and the attendee seeking behavior modification through documentation that is resourcefully dissected at a level that is unsurpassed in this Institute. Each technique (documentation) dissection experience is truly one of the most rewarding things I have done in my life. And I am grateful.
I want to thank Dan Houglum, Torin Berge, Dave Drummer, Jen, Hannah and RJ for their assistance in making this course so enjoyable to teach and apply to “real” life limitations and likenesses.
January 25th was recorded as the second highest daily snowfall in Lincoln of all time, dropping 14.8 inches of snow at a record rate. Between phone calls and emails while working from home, all of us at the Institute were busy “Digging Out”, while at the same time being driven further into a pattern. This same system (of snow) hit much of the Midwest by varying degrees, and many of you, like me, may be feeling the effects after hours spent pushing and plowing our entries back to the outside world. There are many considerations to keep in mind while performing any repetitive, patterned driven activity, and in respect to clearing snow, they are heightened by the exertion and work needed to move the literal mass in front of you. Any activity occurring “in front of you” poses challenges in itself because of the linear forward movement which is often repetitive. Many of these activities and considerations are highlighted in our “Restoring Alternation in Your Daily Lives” Patient Guide which was published last year.
When it comes to pushing snow, be mindful of the following.
When pushing snow on a flat surface, consider first your hand placement and center of mass, in relation to the mass being moved in front of you and the ground below you. The most natural position will be for you to instantly lower your right arm nearest to the blade of the shovel, and your left arm closer to your body. This will lead to your COM to shift over your right leg causing you to work through Right AF IR, Left Trunk Rotation, and Left AF ER positioning, while further driving your pattern.
Instead, consciously start by reversing the above position, lowering your left arm further down the shovel and placing your right arm nearest your body. This will allow your COM to shift to the left, leading to Left AF IR, Right Trunk Rotation, and Right AF ER positioning, while helping to minimize the above pattern. Over time it is likely that you will naturally re-adjust back to the first position as it is what your body is asymmetrically driven to. When possible alternate between these positions as much as possible to minimize some of the common aches and pains that occur from pushing snow in a patterned position!
"The new normal." That’s a phrase we all have heard many times during the last 10 months. As we are all adjusting to what that phrase means to us individually on a personal level, all of us are adjusting to what that means with regards to our relationships with each other as well. We are all finding new boundaries, and freedoms, associated with this "new normal."
PRI opened the 2021 year with the newly revamped Impingement and Instability course, which introduces the concept that impingement and instability are both necessary and vital for optimal human performance. They provide new boundaries and freedoms that allow us to be able to oscillate between our two hemispheres of our body and brain. Our body needs to find a "new normal" with these new parameters in order to appreciate the left side of our body and the right hemisphere of our brain. As I reminded the course attendees, the question isn’t "are you going to get onto your left leg?", the question is "how are you going to get onto your left leg?"
This upgraded course introduces the neuromechanical concepts to answer the question of "how", as this course serves as a gateway into the other PRI Secondary and Tertiary courses, such as Forward Locomotor Movement. This is the material Ron was looking to introduce 20 years ago, and it is my honor to be able to help provide the neurological answers to the question "how are you going to get onto your left leg?" As we discussed during the entirety of the weekend, the how is rooted in one’s ability to compress, or impinge, certain areas of the body, and decompress, or destabilize, other areas of the body. In order for the brain to appreciate these novel concepts, we need to provide the cortex of the brain with novel reference centers for proper inhibition of functional cortical dominance.
As we embarked on our "new normal, " not only in 2021, but in our cerebral cortical function, this course has now become much less of the orthopedic course it had to be several years ago, but has progressed into the neuromechanical blueprint for behavior modification that Ron had intended from Day 1 of the Institute. This course has always been my personal favorite of all the PRI courses offered because it is a clinician’s course as it provided me a more integrated manner to apply the information I had learned in the three PRI introductory courses. My appreciation for this course has grown dramatically due to the necessary evolution from an orthopedic delivery to a neuromechanical, cohesive, and expansive delivery of PRI concepts. As the attendees of the course can attest to, Impingement and Instability helps our body’s ability to appreciate the "new normal" from the inside out.
We are excited to introduce and congratulate our Postural Restoration Trained (PRT) Class of 2021! PRT is the result of completing multiple advanced PRI courses, demonstrating a thorough understanding of the science through completion of the PRT application, and successfully participating in practical and analytical testing. This past weekend, five professionals earned the designation of Postural Restoration Trained (PRT) under the direction of Ron Hruska, Dan Houglum and Jennifer Platt.
The Postural Restoration Institute® established this credentialing process in 2011 as a way to recognize and identify individuals with advanced training, extraordinary interest and devotion to the science of postural adaptations, asymmetrical patterns and the influence of polyarticular chains of muscles on the human body as defined by the Postural Restoration Institute®. The PRT credential is available to Certified Athletic Trainers, Certified Athletic Therapists, Exercise Physiologists and Certified Strength and Conditioning Specialists who have completed the course requirements, application and testing process. With the addition of this class, there are now 59 PRT professionals throughout the U.S and Internationally.
As we approached this New Year, I reflected on the the year that was 2020. As I transitioned into this new role of Executive Director at the beginning of this year, I could have never imagined the challenges we would be facing in just a few short months. I think most people would agree that 2020 was a year that none of us could have ever predicted, but even with the challenges presented from COVID 19, we were determined to make the best of it. And that’s just what we did! The events of 2020 really encouraged us to explore new ways to expand our ‘reach’. Although we already had our primary courses available online, we transitioned quickly to live stream virtual courses for our secondary, tertiary and affiliate courses, and this allowed us to reach interdisciplinary professionals from all over the world. Several live stream courses were sold out with 100 attendees, and many had at least a dozen countries represented. We are grateful that we were able to continue to reach you through PRIVY and podcasts, in addition to some new projects geared towards expanding our reach to the general public, including the ‘Restoring Alternation’ Patient Daily Living Guide. We also took advantage of the circumstances and reached thousands with our ‘PRI Breathing in COVID Times’ 9-week webinar series, which was (and still is) available online for both the general public and healthcare & fitness professionals. The word ‘reach’ has always been a staple of our Institute, and for those of you who are familiar with the PRI non-manual techniques, you have undoubtedly experienced the power of a reach. While our ability to reach you over this past year has been primarily through digital formats, we are excited to get back to reaching (with) you at our live in-person courses. We will be forever grateful for all of you who allowed us to continue to reach you during this crazy, uncertain past year that was 2020. It’s a year that we will never forget, but due to the circumstances that were presented, we now have many new means in which we plan to continue to reach you in 2021 and beyond.
Although we didn’t print a brochure this year, you can see that ‘reach’ would have been the theme carried out within the pages of our Programs and Courses brochure. Please visit our website over the coming year for the most up to date schedule of our programs and courses. In addition to returning to hosting courses across the country this Spring, we are excited to be offerering over 20 live stream courses this year, and we will also have limited in-person attendance available for each of the live stream courses held in Lincoln, Nebraska.
We hope we have the opportunity to reach you, in one way or another, in this New Year!
Every December I reflect on my past year personal and professional activities, a few days before beginning the Advanced Integration course. My inner wellness usually transforms during these four days because of the way I feel connected in real time with real bodies, who have real interest in how our bodies transform by revolving and evolving around axial sagittal verticality and appendicular horizontal integration. I need this eye-level connection with other people to complete my year and to advance myself, as well as the science I am so obsessed with. This past year, as challenging as it was, advanced all of us because we needed to connect with technology in ways that we never have before; to revolve, evolve, and transform with other people.
Technology is value neutral. It becomes value non-neutral, depending how one uses it. The amount of time I spent this last year in some virtual space, or in the space above my neck, by observing bodies above the neck, is overwhelming. However, because of my need to connect with real people, real bodies with real interactive interest, I had to do so with eyes primarily, that were all at eye-level with mine. Body language became eye language.
This opportunity to interconnect, virtually, reduced my isolation and actually advanced me in so many ways. I have never been more prolific or productive, in my life, like I have been this year. New courses composed, books read, research reviewed, interdisciplinary collaboration, etc. all reduced potential obsolescence because of technology. Who would have thought a little virtual reality would advance us, like it has.
Therefore, it just seemed natural, that after a year of virtual wellness, we would host an Advanced Integration course with 11 people (PRC applicants) actually sitting to the left and in front of me and 100 people sitting in a ‘Hollywood Squares’ box, slightly to the right and also, in front of me. It advanced all of us who were in attendance. We received the best of two worlds of advanced postural restoration presence. This advanced technology seemed so value non-neutral challenging, so futuristic, so non-elementary, so alive and yet so unimaginable, because we were all not in the same room and breathing in the same space. Everything we did the year before, now feels so retro.
This December my inner wellness rose to a new, novel and an unnatural high. And I am sure all of the future December PRI Advanced Integration course attendees will reflect on the how “real”, integration feels during these four days, in real time, with real bodies on one side of the room and real faces on the other, all because of value non-neutral technology.
We are excited to announce and congratulate the Postural Restoration Certified (PRC) Class of 2020! PRC credentialing is the result of completing multiple advanced PRI courses, demonstrating a thorough understanding of the science through completion of the PRC application, and successfully participating in practical and analytical testing. This week, 11 clinicians earned the designation of Postural Restoration Certified (PRC) under the direction of Ron Hruska, Lori Thomsen, Dan Houglum, and Jennifer Platt earlier this week.
The Postural Restoration Institute established this certification process in 2004 as a way to recognize and identify those individuals with advanced training, extraordinary interest and devotion to the science of postural adaptations, asymmetrical patterns and the influence of polyarticular chains of muscles on the human body as defined by the Postural Restoration Institute. The PRC credentialing program is available to physical therapists, physical therapist assistants, occupational therapists, and chiropractors who have attended PRI courses, demonstrated a thorough understanding of the science through completion of the PRC application, and successfully participate in both clinical and analytical testing. To date, 226 professionals have earned the designation of Postural Restoration Certified (PRC).
What a fun experience it was to be able to connect with the 37 participants from last month’s live stream pediatrics course! With the new format, we were able to reach attendees in Japan, Canada, Poland, and India! James and I also brought the PRI science to 6 new (“VIP”) clinicians! Further, the audience was made up of yoga instructors, OT’s, personal trainers, and of course, PT’s. The participants seemed to enjoy the many videos of PRI treatment with children of all ages and all skill development levels. We were even able to do some demonstrations with kids! A special shout out to Jen Platt, Nancy Hammond, Libby Lostetter, and anyone else who let us use your children for a spotlighted kid demo! And the adult attendees who participated in demonstrations were also greatly appreciated as it brought a nice richness to the learning experience.
I’ve since been in touch with some of the attendees to see what they thought about the new format and a common comment is how nice it is to have the recording of the class for 10 days following the weekend to go back and review and refresh! It worked out so well, we are planning another Live Stream for August 28-29, 2021 with hopefully a couple in person courses as well. Check out the schedule, and tell your friends! Lastly, huge shout out to co-presenter, James Anderson, producer, RJ Hruska, as well as to Hannah Hankins and Jen Platt for all of the scheduling, manual edits and production, technical help and behind the scenes planning that putting a course like this together requires! And last but not least, thanks to Ron Hruska for the genius foundation! Hope to see you in 2021!
We all have patients that have a tendency to relapse into a previous condition or mode of behavior that was more than likely built around lateralized pattern strength and movement, that affected both horizontal and vertical cycles of compression and decompression at the pelvis, abdomen, thorax, paranasal sinuses and third and fourth ventricles of the cranium. Focusing on reformatting new methods on how to integrate adductors with abductors, internal rotators with external rotators, or flexors with extensors is a challenge in itself, but when someone’s cycles of rhythm are not in synchrony with that effort, the end result of recidivism is more than likely not the result of erroneous effort or program design. It more likely is a representation, to some degree, of the autonomic nervous system’s role in neuromodulation of the patient’s familiar central nervous system’s past effort. Body motor function, in general, has strong somatic nervous system bias, built by positive reinforcement from past voluntary motor patterning. Successful resolvement (self-regulation, self-healing or self-regulation) of this ANS, CNS and SoNS imbalance requires our vagal nuclei and basal ganglia to respond to cyclical oscillatory rhythm, without a response of threat (ergotropic response) from the ANS.
On-going repatterning occurs with every nuance in life. Our asymmetrical design allows us to remain rhythmical because all three of our nervous systems are dealing with input that is received from two sides of the body, that are purposefully designed for different functional cycling; not bicycling but biologic-cycling. Having the opportunity to relate our clinical relapse dilemmas to research that support effort to program activities that harness patterned laterality and cycling threat through cranial freedom from body dependency on the neck, is something I always look forward to.
The 33 virtual attendee’s interaction, through comments and questions forwarded to Jen Platt and directly to me, during this two day course, enhanced the discussion on how the tone of our body is tuned by ANS tension, and how clinical regulation of cyclical flow of air and frequency of sound, can enhance midrange physiologic outcomes for acceptance of novel physical construct. Cathleen deSmet PT, PRC thank you for your inquisitive and thoughtful questioning and verbal reasoning and verbal repeat of the desirable answer we were trying to achieve. It absolutely benefitted every participant. Alice Lam DDS, you have no idea how much I appreciate your attendance and input. It simply helps everyone when you ask a question from a dental perspective. Greer Mackie PT, DPT, your enthusiasm and smile warmed me and reinforced my passion. Jill Maida PT, DPT, MDT, PRC, your title as “oscillatory” queen will remain with you through my eyes for a long time, simply because your presence invokes oscillation. Rachel Smith DPT,PRC your Sunday dialogue on the ‘centric’ elements of patterned autonomic features was so appreciated and kept us all engaged. And finally, Jessica Tidswell PT, ATC,PRT, what can I say about someone who I believe has integrated, is integrating, and will continue to integrate the “laterality” of all three neurologic systems, simply because you were born to do so. I really enjoyed seeing and interacting with this entire class of dedicated autonomic, asymmetric, autonomous minded people and look forward to teaching it again in May of next year.
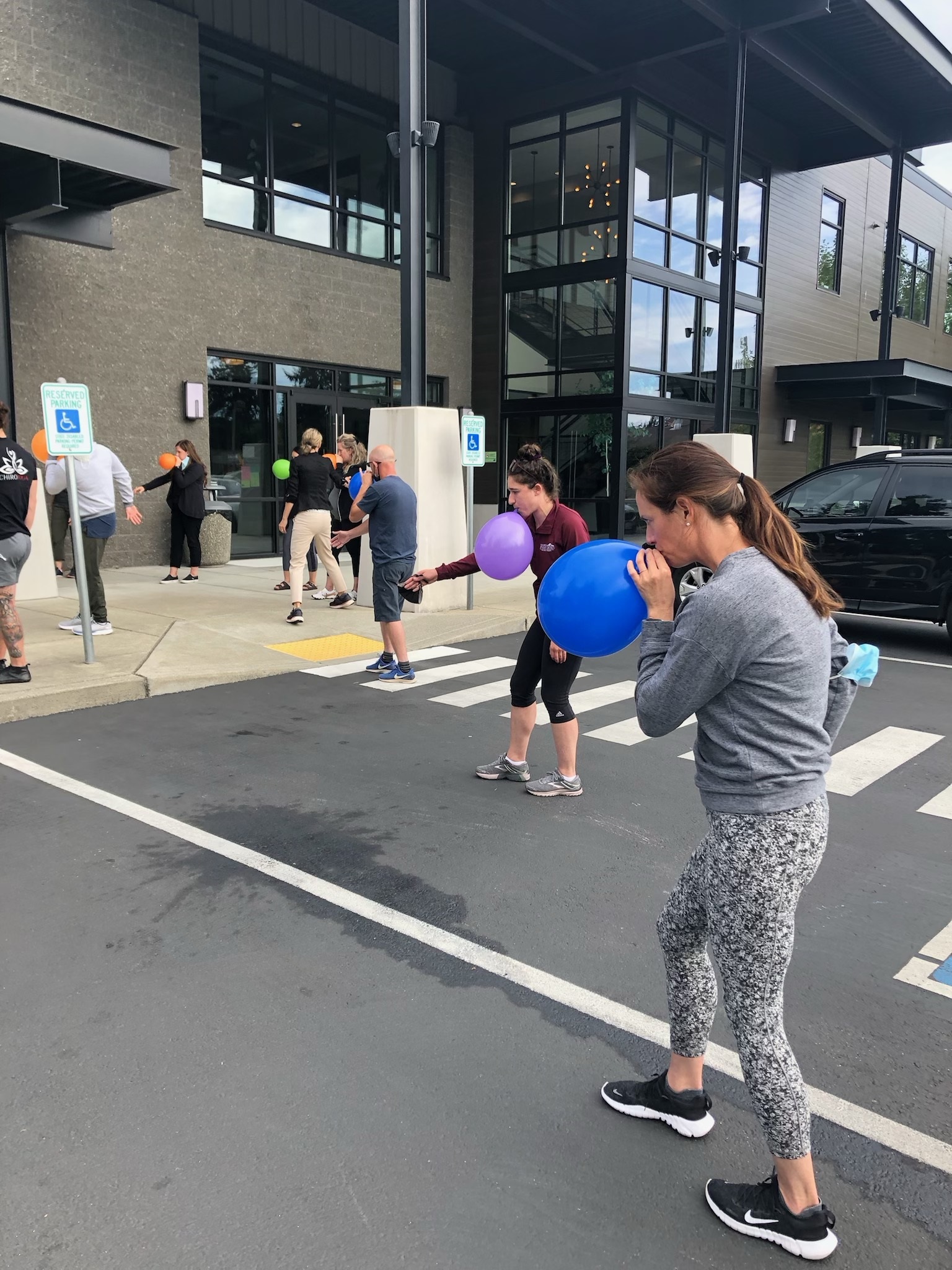
Boy is was good to be back teaching a live course this year. It was food for my spirit to have human interaction and comradery. My fellow colleagues that attended this weekend’s Pelvis Restoration Course were also grateful to be attending a live course as well. We all needed it. We did it safely for our community and each other. We had four professionals attending their first PRI course and several were attending their 3rd course or more this weekend. I feel the class took away the value of the pelvic inlet and outlet positioning needed not only to achieve left stance and right swing, but the value of this positioning to integrate with the respiratory diaphragm in the thorax for the left and right sided hemi-pelvis’ to compress and decompress to allow for Forward Locomotor Movement. Having a smaller class size afforded more personalized lab time for PRI tests, techniques, and practice. It was a fun fun weekend to teach and to learn. Thank you IRG for hosting Pelvis Restoration in Mill Creek.
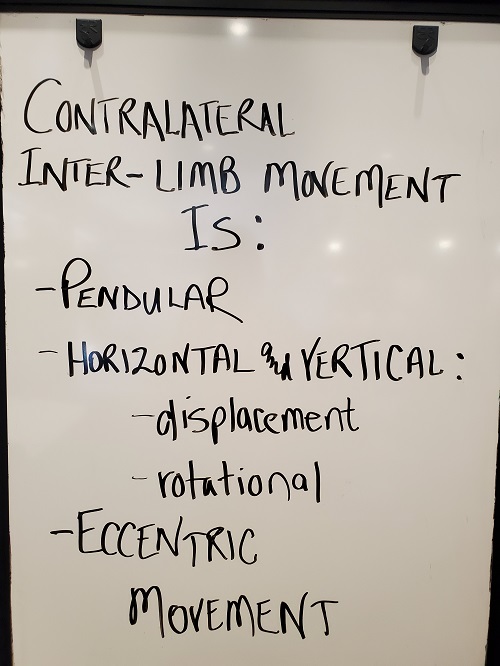
The greatest directional influence on our body’s tensegrity and tempo is forward movement. All of our integration of planar function and neurosensory function is correlated with our environment moving backward; as we cough, speak, walk, reach, chew, listen, sit, watch, etc. The slightest forward movement of the head, arm or leg, is cortically recognized and managed through vestibular related memory and reflex, and cerebellar coordination of the somatic motor sphere. Our ground and space around us are “ours” when we move forward. No one else possesses this personalized biopsychosocial and psychophysiological event. The benefits associated with forward movement, far out weigh those of moving in any other direction. And that would include the wonderful gift of “falling” backward, only to “catch” ourselves, by reaching forward, with a head, arm or leg.
The greatest benefit of having lateralized cortices for integrated visuo-spatial, hemispheric chest, upper limb and lower limb alternation is bipedal, upright forward locomotor movement. Between five million and seven million years ago, some apelike creatures in Africa began to walk habitually on two legs, through savannas, using visuo-spatial propulsion, inter and intra arm pull, and hemi-chest compression. They never could have walked from Africa into Asia and Europe, two million years ago, if they did not first make and flake crude stone tools with their upper limbs, a half million years prior to that time. Their arm function was necessary for their respiratory chest endurance to travel and for their peripheral view as a safe voyager.
The modern form of a human, as we know of today, depended on this earlier pre-existent, hemi-cortical dominance, approximately 200,000 years ago, for refinement of existential forward movement that revolved around the establishment of culture and community. How we shape, grow, pattern and build our behavior and our body, depends on how we move objects that are in front of us and to the side of us, toward us and to the back of us, with inter and intra-limb pull, chest compression, and visuo-spatial propulsion; all allowing us to move forward, like our 200,000 year old ancestors.
(Sarah Petrich, @drsarahpetrich, Instagram)
Our industrial commercialism, capitalism, and careerism, in the present time, has contributed to our heads moving forward, objects in front of us moving forward with us, and objects or environments on the side of us, all moving forward together at some, or all of the time during “walking”. We are on an ecological and evolutionary timeline where the human, in his and her civilization, are doing everything they can to move themselves forward efficiently, in an existential sense. Unfortunately, because of the un-natural commodities around them, they are also moving the entire environment and world around them, with them. Our cortices developed in size because of the need for cortical interplay, as we became dependent on each other, through our sense of movement, space, communication and balance from our eyes and ears, chest walls and cavities and upper and lower limbs. Concrete pavements, straight walls and fast-moving transport systems did not develop today’s unhealthy and unnatural imbalanced forward locomotion. It did however, help bring out the biological rivalry we so often see in our patients, between their two eyes, ears, arms, chests, and legs; and furthermore, contributed to the more recent world of over lateralization for survival of the fittest, fastest and flattest (spine) humans.
(Sarah Petrich, @drsarahpetrich, Instagram)
Homo Sapiens, and the way they move themselves forward, are still evolving and the four components of corollary cortical function are outlined in this course, simply because these four components and the degree to which they are used with and by each other, will reflect on the future’s researcher and anthropologist studies of Holocene human climate of forward movement patterns. Our social climate, our environmental climate and our health climate reflects the demands and challenges we place on our own bodies and thus the environment that encompasses these human patterns of addicted adduction of four of the most precious resources are bodies possess.
I personally, want to thank Jen Platt who consistently and constantly puts up with me and my insane requests to put material together that has never been put together, to my knowledge, in the manner that we have, with outlined research that supports the forward movement, that we should respect. I have been looking forward to teaching a course like this for many years. Therefore, it is hard to summarize my feelings about this topic and the opportunity that this year and the staff around me, presented me. Such a gift. Personal gratification is extended to all you who are observant, and watchful of this journey, of broadening the environment and evolution that is responsible for the patterned world we live with and in, today.
I had the wonderful fortune to visit with Dan Houglum MSPT, ATC/L, PRC the day before this course was presented via live stream, beginning on Aug 22nd. Dan’s insight on the Institute’s past, present and upcoming future is always appreciated and questioned by me, simply because he places events, courses, course material provided in two or more courses, timelines, and approaches in an aligned state, for comparison, contrast and collocation. He and his career time have grown around this juxtaposition. He has an intuitive sense of how organizations operate by addressing and assessing this operational behavior, and therefore, he enjoys watching, and participating in, the delivery of the Impingement and Instability course; that was initially offered in 2007 without the ability of the attendee to compare it to another pre-existing course.
The fact that the first course in February of 2007 can be compared to the last course presented in August of 2020, allows one to quickly see the similarities and the advancements. The fact of two courses, with the same title, written by the same author, can be placed close together with contrasting effects is called a juxtaposition. The juxtaposition of these two courses portray an image of position of bones in 2007 and a position of sense of these same bones in 2020. Dan took his first PRI course in 2004 and has had significant juxtaposition moments since. Juxtaposition is a word that describes the contrasting effect of two things that are placed side by side or close together. For example, two course manuals, with different dates and yet with the same information, may have juxtaposition when one of the courses have been updated, advanced or added onto. Another example of juxtaposition, is this course itself, by looking at cortical function of the human’s two sides of the body that are parallel to each other or “next to each other”. Instability on one side of the body may need to occur when the other side of the body, in the same region, is referencing impingement or the contact of two bony or joint surfaces. One side needs to cortically “loosen” up while the other side can “tighten” up.
This ‘positional juxtaposition’ helps us appreciate the need to experience instability, to remain on guard and prepared, as well as the need to experience impingement, to remain confident and in control, when we lose sense of composure. Parallelism of our two sides of our body, and their associated neurologic and orthopedic juxtapositions, has always been a strong interest of Dan’s, and having him by my side, when I taught this live stream course, gave me and everyone that was present, a considerable amount of favorable comparative contrast.